How Ebola Spreads and How to Protect Yourself and Your Family: Prevention and Safe Practices
by Maroa Noa · 08 Jun 2026
According to the CDC, transmission requires direct contact with infected blood, secretions, or body fluids, or with contaminated objects.
This limited transmission route means that with basic infection control, hand hygiene, barrier precautions, and safe burial practices, transmission can be nearly eliminated.
This article explains how Ebola spreads, who is at risk, and practical prevention strategies for East African families, healthcare settings, and communities.
How Ebola Is Transmitted: Direct and Indirect Routes
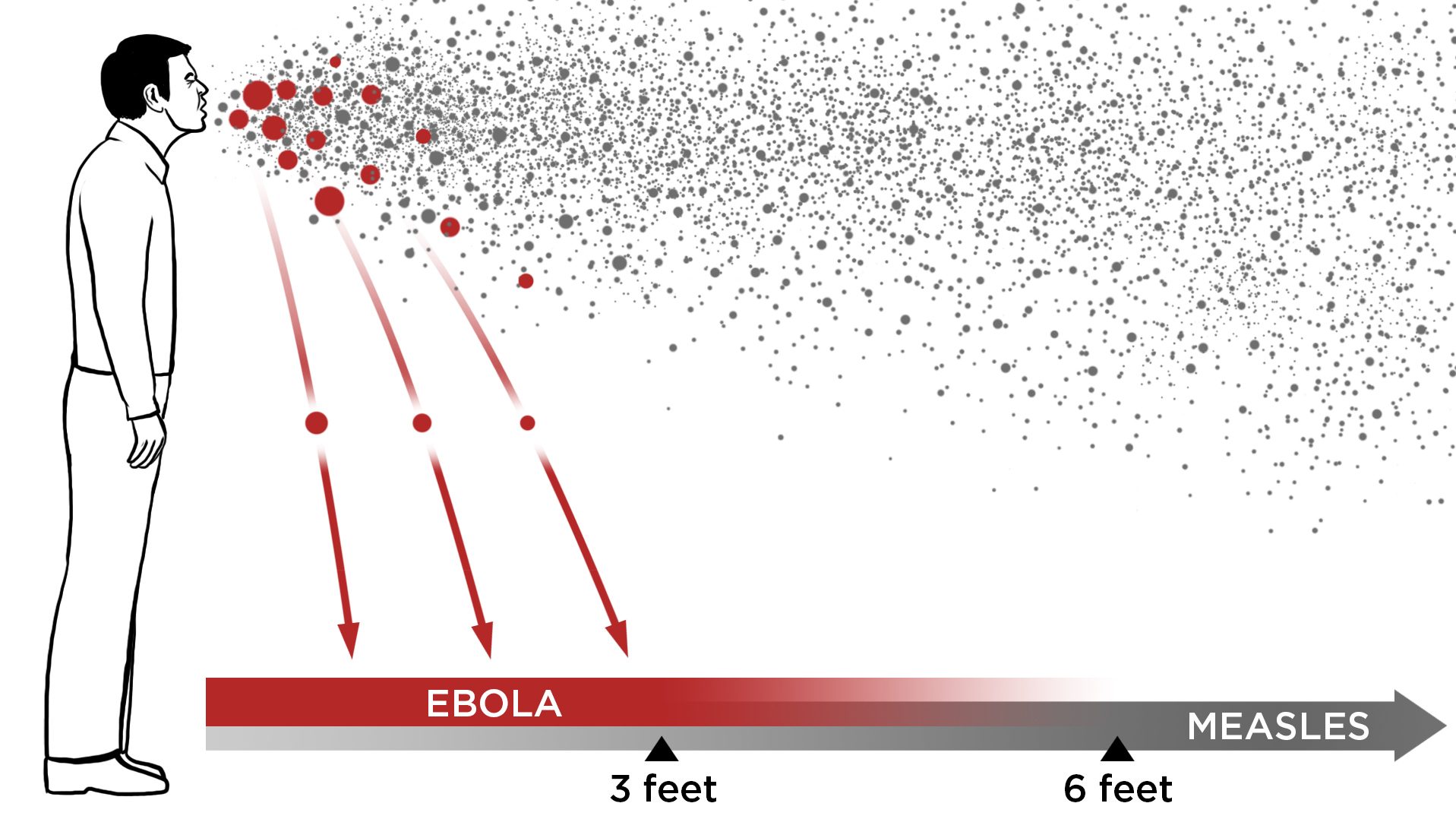
What the CDC Says: Body Fluids, Not Air
The CDC is clear: Ebola does NOT spread through the air like influenza or COVID-19. You cannot catch it by being near someone, breathing the same air, or even having a conversation with an infected person. Instead, the CDC states that transmission requires direct contact with:
|
Route of Transmission |
Details |
Risk Level |
|
Blood of an infected person |
Contact via broken skin or mucous membranes (eyes, nose, mouth) |
Very high if unprotected |
|
Body fluids (saliva, sweat, tears, urine) |
Must contact broken skin or mucous membranes |
High without barriers |
|
Vomit or diarrhoea |
Highly infectious if contact with mucous membranes or broken skin is made. |
High; common in caregiving |
|
Breast milk |
Infected nursing mother to infant; can persist for weeks in survivors |
High in nursing dyads |
|
Semen |
Male survivors can shed the virus in semen for weeks; sexual transmission is possible |
Medium; preventable with a barrier |
|
Contaminated objects |
Needles, bedding, clothing, and medical equipment with blood or body fluids |
High for healthcare workers |
|
Dead bodies |
Direct contact with the body during preparation, funeral, or burial rituals |
High without PPE |
|
Animal contact |
Handling bats, primates, and bushmeat (raw meat from wild animals) |
Moderate; outbreak source |
Entry Points: How the Virus Gets In
The Ebola virus cannot penetrate intact skin. The virus enters the body through:
(1) broken skin, cuts, scrapes, or abrasions;
(2) mucous membranes, eyes, nose, mouth, or genital tissues;
(3) parenteral routes, needle-stick injuries, or injection of contaminated blood.
This is why healthcare workers who use barrier precautions (gloves, gowns) and avoid needle-stick injuries have virtually zero risk, while those without PPE face significant occupational hazards.
Who Is at Highest Risk?
Healthcare Workers & Family Caregivers
The CDC emphasises that healthcare workers and family members caring for Ebola patients WITHOUT proper infection control methods have the highest risk of infection.
During the 2014–2016 West African outbreak, healthcare workers accounted for disproportionately high case numbers. However, healthcare workers with strict PPE adherence had near-zero infection rates, demonstrating that the risk is preventable.
Secondary Transmission in Households
In household settings, transmission typically occurs between symptomatic patients and family members who provide care without PPE, washing the patient, handling soiled linens, or touching the patient's body fluids.
Close physical contact (touching, hugging) is safe only if neither person has open skin lesions. Shared eating utensils, dishes, and bedding do not transmit the virus; what matters is contact with infected body fluids.
Funeral and Burial Practices
Traditional African funeral and burial practices, such as washing the body, touching the deceased, and performing rituals, have been major transmission sources in past outbreaks.
Direct contact with the body of a deceased Ebola patient is extremely high-risk. Safe handling by trained personnel using PPE is essential.
|
💊 PERSONAL PROTECTION & PREVENTION TIPS |
|
If caring for a family member with suspected or confirmed Ebola, wear gloves and a gown when handling the patient, their body fluids, or soiled items; wash hands thoroughly with soap and water after. Do not touch your face or eyes or eat until you have removed your gloves and washed your hands thoroughly. Avoid direct contact with blood or body fluids (vomit, diarrhoea, urine, saliva, sweat). Use plastic or cloth barriers when possible. Clean contaminated surfaces (floors and bedside) with household disinfectant (dilute bleach solution is effective) or approved hospital disinfectant. Do not reuse gloves; dispose of used gloves as infectious waste in a sealed bag. If you have an open cut or skin lesion on your hands, wear two pairs of gloves or cover the wound before caring for a patient. Healthcare workers: use full PPE (gown, double gloves, N95 mask, eye protection, and face shield) for any patient with suspected Ebola; avoid needle-stick injuries by using safety devices. For deceased persons, only trained personnel wearing full PPE should handle the body. Safe burial services should be arranged through your health facility or health authority. |
What Does NOT Spread Ebola
Common Misconceptions Addressed
According to the CDC, you CANNOT get Ebola from the following:
|
Myth |
Fact (CDC Guidance) |
|
Being near an infected person |
Ebola is not airborne; you need direct contact with blood or body fluids |
|
Sharing food or drink |
A virus in saliva only transmits via broken skin or mucous membranes, not the intact digestive tract |
|
Shaking hands or hugging |
Safe if neither person has open skin lesions and no body fluids are exchanged |
|
Breathing the same air |
Not an airborne disease; no risk from shared air |
|
Mosquitoes or other insects |
Ebola does not spread through insect vectors |
|
Contaminated water (drinking) |
A virus does not survive in water; stomach acid destroys it |
|
Pets or casual animal contact |
Domestic animals (dogs, cats) do not carry or transmit Ebola |
|
Sweat alone (if skin intact) |
Must be direct contact with infected blood/body fluids through mucous membranes or broken skin |
Transmission in Healthcare Settings: The Challenge & Solution
Infection Prevention and Control (IPC)
Healthcare facilities in outbreak areas must implement strict IPC measures:
(1) triage, identify suspect cases early, and isolate;
(2) hand hygiene, access to soap, water, and alcohol-based hand sanitiser;
(3) PPE, adequate supply of gowns, gloves, N95 masks, and eye protection;
(4) safe injection practices, using single-use needles with safety devices;
(5) waste management, segregation, and safe disposal of infectious waste;
(6) cleaning and disinfection, routine disinfection of patient-care areas;
(7) environmental controls, negative-pressure isolation rooms if available, or designated isolation wards;
(8) Training: regular training of all staff on correct PPE use and doffing (removal).
Safe Burial Practices: Reducing Transmission After Death
The body of a deceased Ebola patient remains infectious. Safe burial requires:
(1) minimal handling: only trained personnel with full PPE should prepare the body;
(2) rapid burial, ideally within 24 hours;
(3) respectful closure, allowing brief, safe family viewing or participation in modified funeral rituals;
(4) community engagement, working with community and religious leaders to explain why traditional full-contact rituals must be modified during Ebola outbreaks.
Communicating this respectfully is challenging but essential. Health workers should partner with community and religious leaders to develop modified funeral practices that honour the deceased while preventing transmission.
For example, families may accompany the body to the gravesite, offer prayers from a distance, and receive grief counselling but should not wash the body or have direct contact without PPE.
|
🩺 WHEN TO SEEK EMERGENCY CARE: RED FLAGS FOR TRANSMISSION RISK |
|
If you have provided care to a suspected or confirmed Ebola patient without PPE and you are now developing a fever, seek medical care immediately. If you have had direct contact with the body of a deceased Ebola patient and develop fever within 21 days, contact your health facility. If you are a healthcare worker with a needle-stick or sharps injury from a patient with suspected Ebola, seek post-exposure prophylaxis (PEP) evaluation immediately. If a family member dies suddenly with fever and bleeding, do NOT proceed with traditional burial practices without first confirming Ebola is not the cause. Contact your health facility. If you are a burial worker or cemetery staff member and have had unprotected contact with a body suspected of having Ebola, monitor for 21 days and seek care if febrile. If you experience any break in PPE (torn glove or splash to face) while caring for a suspected Ebola patient, wash immediately with soap and water and seek medical evaluation. If you have sexual contact with an Ebola survivor and were not using barrier protection (a condom), seek medical evaluation immediately. If you have been exposed to bushmeat or wild animals in an Ebola-affected area and develop fever, seek care and inform providers of the exposure. |
|
🩺 Clinician Pearl |
|
In the East African context, the challenge is protecting healthcare workers and families while maintaining compassion and cultural sensitivity. Emphasise to your teams and communities: 'Ebola is difficult to catch IF we take precautions, and impossible to catch if we follow them strictly.' Train staff on correct PPE donning and doffing; improper removal causes more infections than patient contact. For family caregivers, provide clear, simple instructions: gloves + barrier = safe. Engage traditional leaders and religious figures early to explain safe funeral practices; rigid rejection of all traditional rituals breeds mistrust. Instead, work together to modify practices that preserve dignity while preventing transmission. In Kenya, the Ministry of Health and county health departments have community liaisons; use them. |
FAQs
1. If someone sneezes on me, can I catch Ebola?
No. The CDC confirms Ebola is not transmitted through respiratory droplets. If someone with Ebola sneezes, the virus in the saliva droplets will not infect you unless those droplets enter a mucous membrane (eyes, nose, or mouth) or open skin.
Even then, exposure is unlikely unless you are very close and droplets contact your face directly. For context, Ebola is less transmissible through respiratory droplets than flu or COVID-19, which DO spread through sneezes and coughs.
2. Can I catch Ebola from kissing someone with the disease?
Potentially, yes, but only if both people have open sores, ulcers, or bleeding in the mouth AND the saliva contains the virus.
If both mouths are intact with no cuts or ulcers and there are no blood or body fluids exchanged, the risk is very low. However, in an outbreak context, kissing is not recommended with anyone with suspected Ebola.
The CDC notes that the risk exists but is much lower than with other routes, like care of a symptomatic patient.
3. Is it safe for healthcare workers to treat Ebola patients?
Absolutely, with proper PPE and training. The CDC states that with strict adherence to infection prevention, a full gown, gloves, an N95 mask, eye protection, and careful hand hygiene, healthcare workers have near-zero risk.
In fact, healthcare workers are NOT at a higher risk than any trained person with proper barriers. The key is consistent, correct use of PPE and strict adherence to safe practices.
Kenya's Ministry of Health has trained over 1,000 healthcare workers in Ebola preparedness and designated treatment teams at KNH and other facilities.
4. Can I help bury a relative who died of Ebola?
Not safe without PPE. If there is suspicion that your relative died of Ebola, you must contact your health facility before proceeding with the burial.
If Ebola is confirmed or suspected, a trained burial team with full PPE will handle the body. However, many facilities allow brief, supervised family participation, for example, standing at a distance while trained workers lower the body into the grave or offering prayers from behind a barrier.
Work with your health facility and community leaders to arrange a respectful, safe closure. The goal is honouring your loved one while protecting family and community.
5. How long can the Ebola virus survive on surfaces or in the environment?
Ebola virus is fragile and is inactivated by heat, drying, disinfectants (including dilute bleach), and ultraviolet light. The virus survives longer in liquid (e.g., blood in a syringe) than on dry surfaces.
On a contaminated surface at room temperature, the virus remains infectious for a limited time, hours to days, depending on conditions.
This is why cleaning and disinfection of patient-care areas with standard hospital disinfectants is highly effective. Household bleach (0.5% solution) is effective and affordable for decontaminating surfaces in homes or low-resource settings.
References
Centers for Disease Control and Prevention. (2026). Ebola disease basics. Retrieved from https://www.cdc.gov/ebola/about/index.html
Centers for Disease Control and Prevention. (2026). How Ebola disease spreads. Retrieved from https://www.cdc.gov/ebola/causes/index.html
Centers for Disease Control and Prevention. (2026). Ebola and Bundibugyo virus frequently asked questions. Retrieved from https://www.cdc.gov/ebola/faq/index.html
Centers for Disease Control and Prevention. (2026). Ebola disease outbreak in the Democratic Republic of the Congo and Uganda [Health Alert Network Notification HAN00530]. Retrieved from https://www.cdc.gov/han/php/notices/han00530.html
European Centre for Disease Prevention and Control. (2023). Factsheet about Ebola disease. Retrieved from https://www.ecdc.europa.eu/en/infectious-disease-topics/ebola-disease/disease-information/factsheet-about-ebola-disease
National Academies of Sciences, Engineering, and Medicine. (n.d.). How does Ebola spread from person to person? Retrieved from https://www.nationalacademies.org/news/how-does-ebola-spread-from-person-to-person
World Health Organization. (2026). Ebola outbreak – DRC 2026. Retrieved from https://www.who.int/emergencies/situations/ebola-outbreak---drc-2026
World Health Organization. (2026). Ebola disease caused by Bundibugyo virus, Democratic Republic of the Congo & Uganda [Disease Outbreak News, 17 May 2026]. Retrieved from https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON602
Centers for Disease Control and Prevention. (2024). Ebola factsheet. Retrieved from https://www.cdc.gov/ebola/media/pdfs/2024/05/ebola-factsheet-P.pdf
Occupational Safety and Health Administration. (2024). Ebola – Control and prevention. Retrieved from https://www.osha.gov/ebola/control-preventio