What Is Ebola? Understanding the Virus, Its Types, and Why the 2026 Outbreak Is Different
by Maroa Noa · 08 Jun 2026
|
📌 KEY TAKEAWAYS |
|
Ebola is caused by one of four orthoebolaviruses (species of virus); the 2026 outbreak is caused by the Bundibugyo virus, which has no approved vaccine or specific treatment. Symptoms appear 2–21 days after exposure (average 8–10 days) and progress from 'dry' (fever and fatigue) to 'wet' (diarrhoea, vomiting, and bleeding) symptoms. Early Ebola symptoms mimic common East African illnesses like malaria and typhoid, delaying diagnosis; healthcare workers must maintain high clinical suspicion. Bundibugyo virus carries a 25–50% death rate, lower than Zaire Ebola but comparable to the previous 2007 and 2012 outbreaks. Kenya and the East African region face a moderate risk due to proximity to DRC/Uganda; border surveillance and community awareness are critical. |
Introduction
Ebola virus disease (EVD) is a rare but severe illness that has captured global attention, particularly with the 2026 outbreak in the Democratic Republic of the Congo (DRC) and Uganda.
Despite its fearsome reputation, understanding what Ebola is, how it spreads, how it manifests, and how it differs from other diseases is essential for both patients and healthcare workers in East Africa.
This article explains the biology of the Ebola virus, the four main types that can infect humans, and why the current outbreak caused by the Bundibugyo virus presents a unique public health challenge.
Ebola virus disease, formally known as Ebola haemorrhagic fever (EHF), has occurred primarily in sub-Saharan Africa since 1976. However, the 2026 outbreak is remarkable: it is caused by Bundibugyo virus, a species for which there is no approved vaccine or specific treatment available.
This outbreak has prompted the World Health Organization to declare a Public Health Emergency of International Concern (PHEIC) and has heightened concern across East Africa, including Kenya, which shares regional connectivity with the outbreak epicentre.
For Kenyan healthcare workers, patients, and the public, accurate knowledge of Ebola, what it is, how it differs from other febrile illnesses, and why the 2026 outbreak is different is vital for early recognition, appropriate infection control, and informed decision-making during this regional health crisis.
What Is Ebola? The Virus and Its Family
Ebola virus disease is caused by a group of viruses called orthoebolaviruses (formerly known as ebolavirus). These are negative-sense, single-stranded RNA viruses belonging to the Filoviridae family, which also includes the Marburg virus.
The name "Ebola" comes from the Ebola River in the DRC, where the virus was first discovered in 1976 during simultaneous outbreaks in Sudan and what is now the Democratic Republic of the Congo.
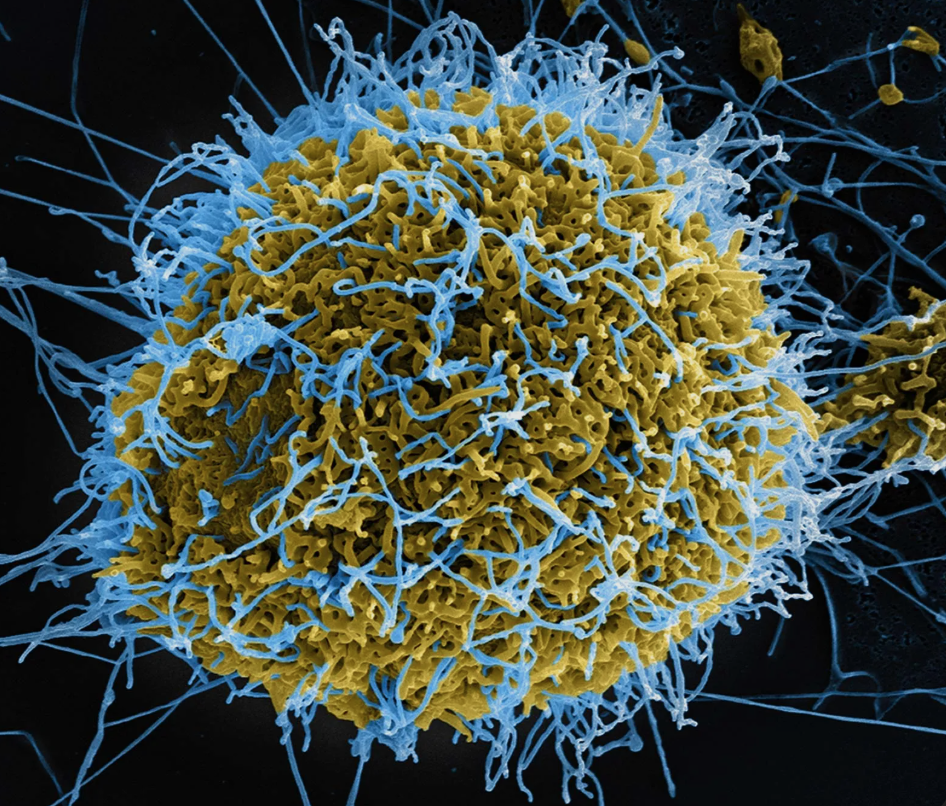
The virus is filamentous and enveloped, meaning it is wrapped in a lipid (fatty) membrane studded with viral proteins.
This envelope is fragile and easily damaged by heat, disinfectants, and drying—a point of critical importance for infection prevention. Orthoebolaviruses are found primarily in sub-Saharan Africa and are believed to originate from wildlife reservoirs, particularly fruit bats, which can carry the virus without becoming severely ill.
The Four Species of Ebola That Affect Humans
According to the CDC, there are four orthoebolaviruses (species) known to cause illness in humans:
|
Species |
Scientific Name |
Key Notes |
|
Ebola virus |
Orthoebolavirus zairense (EBOV) |
Most common; highest death rate (50–90%); largest outbreaks |
|
Sudan virus |
Orthoebolavirus sudanense (SUDV) |
25–50% mortality; has caused sporadic outbreaks since 1976 |
|
Bundibugyo virus |
Orthoebolavirus bundibugyoense (BDBV) |
25–50% mortality; rare; 2026 outbreak in DRC/Uganda; NO vaccine/treatment |
|
Taï Forest virus |
Orthoebolavirus taiense (TAFV) |
Rare; only one recorded human case; non-fatal |
Note: Two other orthoebolaviruses exist (Reston virus and Bombali virus) but have not caused significant human disease. Though they have caused disease primarily in non-human primates, or have unclear pathogenicity in humans.
The 2026 Bundibugyo Outbreak: Why It's Different
The current outbreak in the DRC and Uganda is caused by Bundibugyo virus (BDBV), a rare species that has not circulated widely in human populations.
As documented by the WHO and CDC, Bundibugyo virus has been recorded in only three outbreaks: Uganda (2007–2008), DRC (2012), and the current 2026 outbreak. The uniqueness of this outbreak lies in the absence of approved countermeasures.
According to WHO guidance issued on 28 May 2026, there is currently no licensed vaccine or specific antiviral treatment for Bundibugyo virus disease. Investigational candidates—including monoclonal antibodies (maftivimab, MBP-134) and antivirals (remdesivir, obeldesivir)—are being prioritised for clinical trials, but none are yet approved.
The only licensed Ebola vaccine, Ervebo, is designed for Zaire ebolavirus and has very limited (and currently insufficient) evidence for cross-protection against Bundibugyo virus. This creates a clinical and public health challenge: frontline responders, contacts, and healthcare workers must rely on infection prevention and control (IPC), supportive care, and surveillance rather than specific therapeutics.
Signs and Symptoms of Ebola
Incubation Period and Early Presentation
According to the CDC, symptoms of Ebola typically appear 2 to 21 days after exposure to the virus, with an average onset of 8 to 10 days.
During this incubation period, an infected person shows no symptoms and is not contagious. Importantly, once symptoms begin, the person becomes contagious.
The early phase of Ebola illness is often called the 'dry' symptom phase and presents with non-specific signs that are easily confused with other common East African illnesses such as malaria, typhoid fever, and meningococcaemia.
CDC data from the 2014–2016 West African outbreak showed that the most common early symptoms include fever (87% of cases), fatigue (76%), vomiting (68%), diarrhoea (66%), and loss of appetite (65%).
Progression: 'Dry' to 'Wet' Symptoms
After 4–5 days of illness, patients may progress to the 'wet' phase, characterised by gastrointestinal and haemorrhagic symptoms. The CDC notes that these include severe watery diarrhoea, vomiting, abdominal pain, nosebleeds, and bleeding into stools or vomit. Importantly, not all patients develop bleeding; thus, the absence of haemorrhagic signs does not rule out Ebola.
Patients with fatal disease typically develop more severe clinical signs early and die of multiorgan failure and septic shock between days 6 and 16 of illness. Non-fatal cases may show improvement around day 6, though convalescence can be prolonged.
Timeline and Symptom Phases
|
Phase |
Timeline |
Symptoms ('Dry' or 'Wet') |
|
Incubation |
2–21 days (avg. 8–10 days) |
No symptoms; not contagious |
|
Early ('Dry') Phase |
Days 1–5 of illness |
Fever, headache, muscle aches, fatigue, loss of appetite, chills |
|
Progressive ('Wet') Phase |
Days 5–10+ |
Severe diarrhoea, vomiting, abdominal pain, rash, nosebleeds, bleeding gums, bloody stools/vomit |
|
Critical Phase |
Days 6–16 |
Multiorgan involvement, shock, death (or slow recovery if survived) |
How Ebola Is Diagnosed
Diagnosis of Ebola requires laboratory confirmation. In healthcare settings across East Africa, including Kenyan facilities such as Kenyatta National Hospital (KNH) and other county hospitals, suspected Ebola cases should trigger immediate infection prevention protocols and rapid specimen collection.
The standard diagnostic test is RT-PCR (reverse transcription polymerase chain reaction), which detects viral RNA. The CDC and WHO recommend that any suspected case be isolated and tested urgently.
A critical issue with the 2026 outbreak: GeneXpert MTB/RIF (or similar platforms commonly deployed for tuberculosis screening) detects Zaire ebolavirus but NOT Bundibugyo virus.
This detection gap has delayed case confirmation and isolation in the DRC and Uganda, highlighting the importance of specific laboratory capacity and communication with the national public health authority.
|
🩺 When to Suspect Ebola: Clinical Pearl for East African Healthcare Workers |
|
Any patient presenting with fever (≥38°C) plus at least three of the following within 21 days of exposure to a known outbreak area: headache, vomiting, diarrhoea, abdominal pain, muscle pain, weakness, or unexplained bleeding. Key risk factors in outbreak contexts: direct contact with a symptomatic person (alive or dead); breach in IPC (needle-stick, splash to mucous membranes); contact with bushmeat or animals found sick/dead; or participation in unsafe burial practices. Early symptoms are non-specific and overlap with malaria, enteric fever, and dengue, common in East Africa. Maintain a high index of suspicion in outbreak-affected areas and test early. Remember: asymptomatic individuals are NOT contagious. Do not isolate contacts without fever; instead, monitor temperature daily for 21 days. If a test is negative on days 1–2 but clinical suspicion remains high, repeat testing is recommended because early-stage viral loads can be below the detection threshold. |
Management and Treatment
To date, there is no specific approved antiviral drug or vaccine for the Bundibugyo virus. Management of suspected or confirmed Ebola cases is primarily supportive and centres on maintaining physiological stability, preventing complications, and strict infection control.
Treatment includes aggressive fluid and electrolyte replacement (for the severe diarrhoea), management of sepsis, blood transfusion if indicated, and organ support. Investigational therapeutics are being evaluated in clinical trials with the affected governments' cooperation.
The WHO has identified three priority compounds for clinical evaluation: MBP-134 and maftivimab (monoclonal antibodies) and remdesivir (antiviral). These are NOT yet approved for use outside of clinical trials.
Vaccines for Ebola: Current Status in 2026
As of May 2026, the WHO has advised that the only licensed Ebola vaccine, Ervebo (rVSV-ZEBOV), is approved for Zaire ebolavirus and is NOT licensed for Bundibugyo virus.
Although laboratory and animal studies suggest possible partial immune cross-reactivity, evidence is very limited and insufficient to recommend routine use of Ervebo for Bundibugyo protection. WHO guidance (28 May 2026) advises against relying on Ervebo for this outbreak.
Candidate vaccines under development for Bundibugyo include ChAdOx1 Bundibugyo (Oxford University/Serum Institute of India), which could potentially be available for efficacy assessment within 2–3 months. However, these remain investigational and are not yet deployed.
|
💊 SUPPORTIVE CARE AND PREVENTION TIPS |
|
There is NO specific medication to kill the Ebola virus as of May 2026. Supportive care includes IV fluids, electrolyte correction, blood transfusion, and organ support. Investigational monoclonal antibodies (maftivimab and MBP-134) and antivirals (remdesivir and obeldesivir) are being evaluated in clinical trials only; do not use them outside trials. Paracetamol (acetaminophen) can be used for fever and pain; NSAIDs are generally avoided to reduce bleeding risk. NO approved vaccine for the Bundibugyo virus is available. The Ervebo vaccine (Zaire-specific) is NOT recommended for this outbreak. Prevention is the cornerstone: avoid contact with body fluids, practise hand hygiene, use PPE if caring for patients, and avoid bushmeat or contact with wildlife. For healthcare workers, full PPE (gown, gloves, eye protection, and N95 mask) is mandatory. Needlestick prevention is critical—this is the highest-risk exposure for HCWs. Supportive care is best provided in settings with isolation capacity (negative-pressure or cohort nursing in barrier facilities). Post-exposure prophylaxis with investigational antivirals (e.g., obeldesivir) is under evaluation but not yet approved for routine use. |
|
🩺 WHEN TO SEEK EMERGENCY CARE |
|
Any fever (≥38°C) plus headache, muscle aches, or fatigue within 21 days of being in an active Ebola outbreak area or contact with a suspected case. Unexplained vomiting, diarrhoea, or abdominal pain, especially if accompanied by fever. Any signs of bleeding: nosebleeds, bleeding gums, blood in vomit or stool, unexplained bruising, or rash. Severe weakness, inability to stand, or confusion. Any healthcare worker or contact of a suspected Ebola case who develops a fever must immediately isolate and report to their public health authority. If you have returned from the DRC, Uganda, or another affected area in the past 21 days and develop any fever, contact your local health facility or call the Ministry of Health emergency hotline (in Kenya: +254 711 959 959 or visit www.health.go.ke). Families or contacts of a deceased person suspected of having Ebola should NOT participate in traditional burial practices that involve contact with the body. Safely handled burials (under supervision) are critical for outbreak control. Do NOT self-treat at home; do NOT share needles or eating utensils with a febrile person in an outbreak area; and do NOT delay seeking professional care. |
FAQs
1. Can you catch Ebola from the air, like the flu or COVID-19?
No. The CDC confirms that Ebola does NOT spread through the air. You cannot catch it by being near someone or breathing the same air.
Ebola spreads only through direct contact with blood or body fluids (saliva, sweat, vomit, diarrhoea, urine, or semen) of a person who is sick with Ebola or has died from it, or through contact with contaminated objects like needles or bedding. This is why isolation and barrier precautions are so effective.
2. If I have been to the DRC or Uganda, should I be worried about Ebola?
If you have been in an affected area (Ituri Province in the DRC or parts of Uganda) within the past 21 days and develop ANY fever, you should seek medical care immediately and inform your healthcare provider of your travel history. However, Ebola remains rare.
The CDC reports that cases are concentrated in specific regions; casual contact with the general public in unaffected areas carries minimal risk. Monitor your health for 21 days: if you develop a fever, headache, muscle aches, or other symptoms, contact your health facility. Many other febrile illnesses (malaria and typhoid) are far more common in East Africa.
3. Why is there no vaccine or treatment for the Bundibugyo virus yet?
Bundibugyo virus is rare. Previous outbreaks occurred in 2007–2008 (Uganda) and 2012 (DRC), so vaccine and antiviral development for this species has not been a priority until this 2026 outbreak.
The 2026 outbreak was declared a public health emergency on 17 May 2026, triggering rapid research efforts.
The WHO notes that candidate vaccines and antivirals are being prioritised for clinical trials, but development, safety testing, and regulatory approval take time. In the meantime, prevention through infection control is the mainstay of response.
4. What is the death rate for the Bundibugyo virus?
According to the CDC, previous Bundibugyo outbreaks had case fatality rates of 25% (Uganda 2007–2008) and 50% (DRC 2012).
The 2026 outbreak death rate is still being assessed, as it is ongoing. For comparison, Zaire ebolavirus (the most common species) has fatality rates of 50–90%. This means that with supportive care, many patients with Bundibugyo virus do survive, provided they receive early treatment, fluid replacement, and management of complications.
5. What should I do if someone in my family shows signs of Ebola?
If a family member or contact develops a fever and has been exposed to a suspected or confirmed Ebola case or has recently returned from an affected area, do the following:
(1) Isolate the person in a separate room if possible, away from others.
(2) Avoid direct contact with their blood or body fluids; use a barrier (gloves, cloth) if you must touch them.
(3) Contact your local health facility or call the Kenya Ministry of Health emergency line immediately—do NOT take them to a general outpatient clinic without prior warning.
(4) Do NOT participate in the burial of a deceased person until safety protocols have been confirmed.
(5) Follow up with your own health facility for monitoring and testing if you have had contact. Early reporting and professional care save lives.
References
Centers for Disease Control and Prevention. (2026). Ebola disease basics. Retrieved from https://www.cdc.gov/ebola/about/index.html
Centers for Disease Control and Prevention. (2026). Clinical features of Ebola disease. Retrieved from https://www.cdc.gov/ebola/hcp/clinical-signs/index.html
Centers for Disease Control and Prevention. (2026). Ebola and Bundibugyo virus frequently asked questions. Retrieved from https://www.cdc.gov/ebola/faq/index.html
Centers for Disease Control and Prevention. (2026). Ebola disease outbreak in the Democratic Republic of the Congo and Uganda [Health Alert Network Notification HAN00530]. Retrieved from https://www.cdc.gov/han/php/notices/han00530.html
Centers for Disease Control and Prevention. (2026). Ebola outbreak: Current situation. Retrieved from https://www.cdc.gov/ebola/situation-summary/index.html
World Health Organization. (2026). Experts convened by the WHO advise on candidate treatments and vaccines for Ebola disease caused by the Bundibugyo virus [News Release, 28 May 2026]. Retrieved from https://www.who.int/news/item/28-05-2026-experts-convened-by-who-advise-on-candidate-treatments-and-vaccines-for-ebola-disease-caused-by-bundibugyo-virus
World Health Organization. (2026). WHO emergency guidance on the use of a licensed Ebola virus vaccine during Bundibugyo virus disease outbreaks, 28 May 2026. Retrieved from https://doi.org/10.2471/B09772
World Health Organization. (2026). Ebola disease caused by Bundibugyo virus, Democratic Republic of the Congo & Uganda [Disease Outbreak News, 17 May 2026]. Retrieved from https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON602
World Health Organization. (2026). Ebola outbreak – DRC 2026. Retrieved from https://www.who.int/emergencies/situations/ebola-outbreak---drc-2026
World Health Organization. (2026). Ebola: Disease information. Retrieved from https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/norms-and-standards/vaccine-standardization/ebola